 By: Dr. Louis H. Berman, DDS, FACD, Endodontist
By: Dr. Louis H. Berman, DDS, FACD, Endodontist
When proper endodontic techniques are used, the success rate for endodontic procedures is just as high as implant procedures. That said, reinfections after endodontic procedures can be frustrating. Although missed canals and improper canal cleaning and obturation are certainly causes, coronal leakage and root fractures lead to most endodontic failures.
Proper hygiene and well-fabricated restorations can help prevent coronal leakage, but root fractures can be a real enigma. Excessive canal enlargement and obturation forces are big contributors to root fractures. However, unrecognized root fractures are often present even before endodontic treatment.
Recognizing root fractures early is very important. Undiagnosed, a root fracture can not only cause endodontic treatment to fail, it also can be responsible for extensive periradicular bone loss, which can compromise a future implant. Diagnostic prowess and good radiographic assessments are paramount in determining if a root fracture is present, especially prior to endodontic treatment.
The Importance of a Pre-Treatment Assessment
Let’s start with a pre-treatment assessment and a few simple concepts the dental literature has given us. The most common tooth in the mouth to have vertical root fractures is the lower second molar. Therefore, before considering endodontic treatment, especially on a lower second molar, you should use some good common sense diagnostic tools and be aware of some interesting findings in the dental literature.
The most common place to see a root fracture is on the marginal ridges, especially the distal marginal ridge. Good magnification and transillumination are very helpful. In addition, in a case whereby the pulp is non-vital, the clinician should always ask: WHY is that pulp non-vital?
Consider a situation whereby the pulp is non-vital, with or without radiographic evidence of periapical bone loss. Was there gross caries or a large restoration in the tooth? What if there was NO restoration or caries in the tooth? IF that were the case, WHY was the pulp non-vital?
This should point the clinician to consider the tooth has a vertical root fracture and is the cause of the root fracture. The root might not be “split,” and the clinician might not be able to visualize the fracture. But in the absence of any other observed etiology, the clinician should consider that a root fracture is present and the prognosis for the pending endodontic treatment might not be favorable, which is known as “fracture necrosis” (Figure 1).

Figure 1: Undiagnosed root fracture in the lower second molar. Note non-vital pulp with periapical/periradicular bone loss, and no restoration or caries. The clinician should question WHY the pulp became non-vital. With no other objective etiology, a vertical root fracture should be considered.

Figure 1a: Pre-treatment radiograph of a virgin tooth with pulp necrosis.
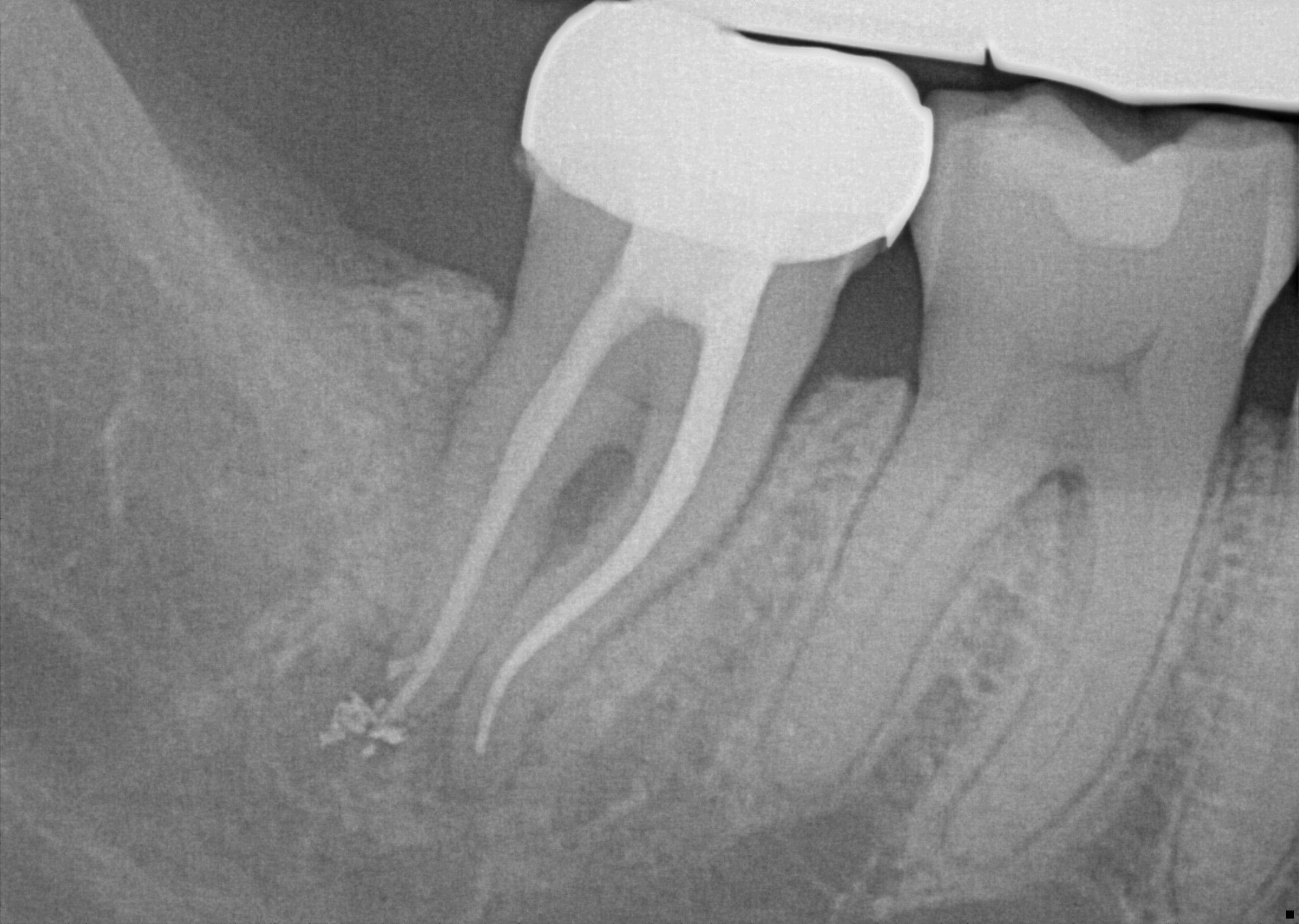
Figure 1b: Radiograph of the endodontic treatment of the virgin tooth.
The Power of CBCT Scans
Radiographs and CBCT are valuable diagnostic tools to help you determine the presence of a root fracture. Unfortunately, unless the fracture is wider than about .15 mm (the tip of a #15 endodontic file), it cannot be visualized on the CBCT scan. However, there are some strong associations between radiographic findings and the presence of a root fracture. Specifically, when the bone loss presents in “J” shaped pattern, it is highly suggestive that a root fracture is present. Often, this can be seen on a two-dimensional periapical radiograph with the bony lesion typically extending from the apex to the crestal bone, sometimes resulting in a deep and narrow isolated periodontal pocket. Sometimes this pocket cannot be probed because it occurs in the interproximal area.
Taking radiographs in the area of the lower second molars can be challenging, especially with patient compliance (sometimes the tooth is “way back there” and may be uncomfortable for the patient).
In addition, consider this: lower second molars are typically positioned in the cancellous bone, almost directly in the middle of the buccal and lingual cortical bony plates. When pulp necrosis becomes infected, the subsequent bone loss is only observed on a periapical radiograph when the bone loss reaches the junction of the cancellous and cortical bone. This makes the radiographic diagnosis of pulp necrosis difficult, especially for the lower second molar. That’s where CBCT can become essential in determining periapical or periradicular bone loss (Figure 2).

Figure 2a: Radiograph of tooth with a root fracture, but not observed in the periapical radiograph.

Figure 2b: Same tooth with a CBCT scan showing periradicular bone loss from the crestal bone to the apex, which is highly suggestive of a vertical root fracture.
Find Fractures Early for Better Outcomes
Endodontic procedures are performed to remove diseased pulp and promote periapical healing. The root canal procedure ultimately provides the foundation for a final restoration.
The endodontic treatment and subsequent full coverage restoration can be expensive for patients; therefore, proper pre-treatment assessment is imperative. Often, the undiagnosed root fracture can cause the endodontic treatment to fail even before the endodontic treatment is initiated. Proper pre-treatment diagnosis, common sense, and clinician intuition will help patients avoid unnecessary treatment by recognizing root fractures in their most early stages.




